Proteinuria is a condition characterised by the presence of greater than normal amounts of protein in the urine. It is associated with a variety of different diseases and is sometimes seen in those who are apparently healthy. Mild or transient proteinuria may become more severe over time.
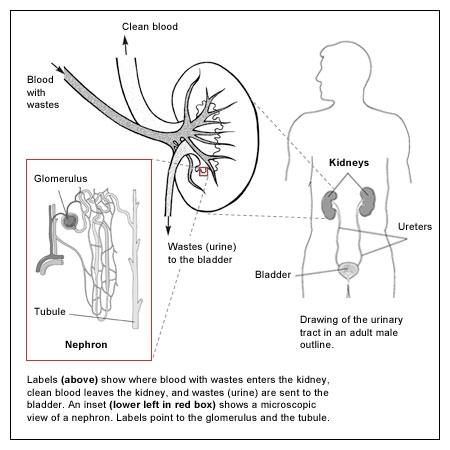
Plasma, the liquid portion of blood, contains many different proteins. One of the many functions of the kidneys is to retain plasma protein so that it is not excreted along with waste products when urine is produced. There are two mechanisms that normally prevent protein from passing into urine: (1) the glomeruli in the kidney provide a barrier that keeps most larger plasma proteins inside the blood vessels but allows water and small proteins to be filtered out and (2) the small proteins that do get through are almost entirely reabsorbed by the tubule.
Proteinuria most often occurs when either the glomeruli or tubules in the kidney are damaged. Inflammation and/or scarring of the glomeruli can allow increasing amounts of protein and sometimes red blood cells (RBCs) to leak into the urine. Damage to the tubules can prevent protein from being reabsorbed, meaning proteinuria may also develop when the tubules cannot reabsorb all of a small protein which has been filtered from the blood.
A variety of diseases and conditions can cause kidney damage which can result in proteinuria. Two of the most common causes are:
Others causes include:
- immune disorders (e.g. systemic lupus erythematosus (SLE), IgA nephropathy, Goodpasture’s syndrome)
- infections
- exposure to toxins
- trauma
- kidney cancer
- pre-eclampsia
- multiple myeloma
Pregnant women are frequently screened for proteinuria because its development is associated with pre-eclampsia (also know as toxaemia), a hypertensive disorder that can cause oedema, nausea, and headaches during pregnancy. Pre-eclampsia can be dangerous for both the mother and her baby.
Proteinuria due to the presence of excess small proteins in blood may be seen in multiple myeloma (free immunoglobulin light chains) and in conditions that damage red blood cells in the circulation and release of haemoglobin which appears with its red colour in the urine.
Healthy people can have short term or long term proteinuria. It is associated with stress, exercise, fever, aspirin therapy, and exposure to cold. Some people excrete more protein into the urine when they are standing up than when they are lying down (orthostatic proteinuria).
Signs and symptoms
Frequently, no symptoms are seen with proteinuria, especially in mild cases. Large amounts of protein may cause the urine to appear foamy. Loss of large amounts of protein from the blood can affect the body’s ability to regulate fluids, which can lead to swelling in the hands, feet, abdomen and face. When symptoms are present, they are usually associated with the condition or disease causing proteinuria.