Allergies (also known as ‘hypersensitivities’) are overreactions of the immune system to substances that do not cause reactions in most people. Hypersensitivities are grouped into four types, I, II, III and IV. These classifications are based on what parts of the immune system are activated and how long it takes for a reaction to occur.
The two types of hypersensitivities commonly associated with the term ’allergies’are type I or ‘immediate’ hypersensitivities, and type IV or ‘delayed’ hypersentivities.
In type I hypersensitivity, a particular foreign substance (known as an 'allergen') reacts with a specific type of antibody called immunoglobulin E (IgE) – this reaction causes symptoms to appear within minutes. In type IV hypersensitivity, the allergen reacts with a specialised type of cell called a T-lymphocyte. In this case symptoms take hours to days to appear.
Type I hypersensitivities affect mainly the respiratory system (nose, throat, lungs), the gastrointestinal system (stomach, intestines, bowel) and the skin. They occur most frequently in those with a family history of allergies (although not always to the same substance). The first time a predisposed person is exposed to a potential allergen, they will not have a major reaction; instead, they will create a specific IgE antibody and become 'sensitised'.
If that person is then exposed to the allergen again, the specific IgE identifies the allergen, attaches to it, and triggers the release of chemicals, including histamine, that cause allergic symptoms. These symptoms start wherever the allergen was introduced (for example in the mouth, nose or on the skin).
On the skin, an acute type I allergic reaction can cause a urticarial rash, dermatitis, and itching, while in the long term the allergy may cause atopic dermatitis and eczema. In the respiratory tract, the acute allergic reaction causes coughing, nasal congestion, sneezing, throat tightness, and, in the long term asthma. It can also cause red itchy eyes. Acute allergic reactions in the gastrointestinal system start in the mouth with tingling, itching, a metallic taste, and swelling of the tongue and throat, followed by abdominal pain, muscle spasms, vomiting and diarrhoea, over time leading to a variety of gastrointestinal problems.
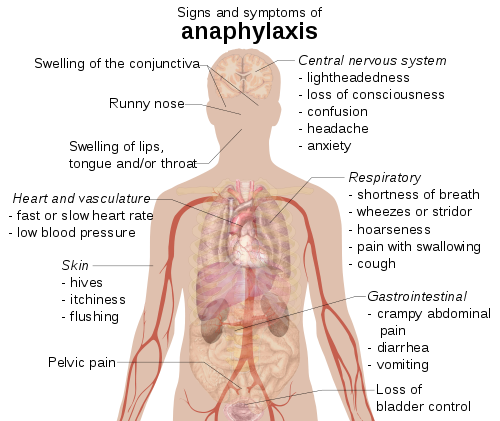
Any severe acute allergic reaction also has the potential to be life threatening, causing anaphylaxis, a reaction spread throughout the entire body that can start with agitation, a 'feeling of impending doom' pale skin (due to low blood pressure), and/or loss of consciousness (fainting). Anaphylaxis can be fatal without the rapid administration of an adrenaline injection.
Type I allergic reactions can be variable in severity, one time causing a rash, the next time anaphylaxis. Type I allergies can be to just about anything: foods, plants (pollens, weeds, grasses, etc), insect venoms (for example wasp or bee stings), animal dander (from the fur of cats and dogs), dust mites, mould spores, occupational substances (for example latex), and drugs (such as penicillin). There can also be cross-reactions, where someone allergic to grass pollen, for instance, may also react to melons and tomatoes. The most common food-related causes of severe anaphylactic reactions are peanuts, tree nuts (such as walnuts and hazelnuts), and shellfish.
Type IV delayed hypersensitivity reactions are most often skin reactions. Common examples include reactions to metal and jewellery. They occur when an allergen interacts with specific T lymphocytes. No immune system ’sensitisation’ is necessary; patients can have a type IV reaction with the first exposure. Type IV hypersensitivity is usually a reaction (redness, swelling, hardening of the skin, rash, dermatitis) observed at the exposure site hours to days after exposure.